| 规格 | 价格 | 库存 | 数量 |
|---|---|---|---|
| 50mg |
|
||
| 100mg |
|
||
| 250mg |
|
||
| 500mg |
|
||
| 1g |
|
||
| Other Sizes |
|

| 体外研究 (In Vitro) |
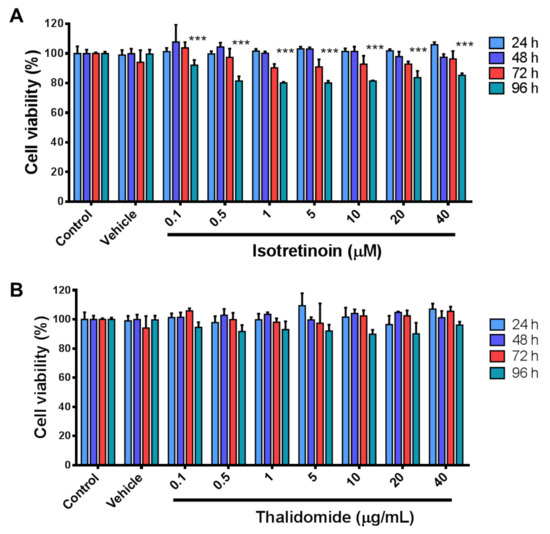
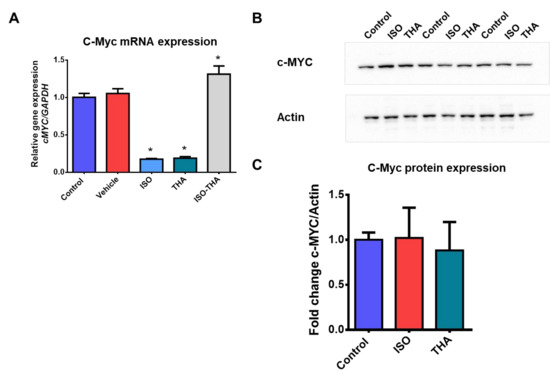
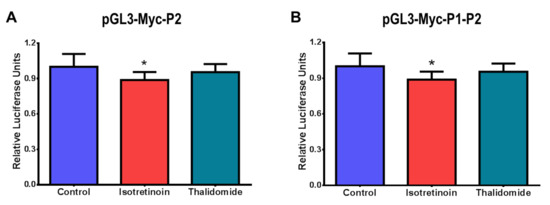
作为一种前药,异维A酸(13-顺式视黄酸)在细胞内转化为代谢物,与核受体 RAR 和 RXR 激动性结合 [1]。异维A酸对光、热和空气的敏感性相当大[3]。异维A酸(0–40 μM;24-96 小时)会显着抑制 HepG2 细胞活力 [4]。 P1 或 P2 启动子活性有助于异维A酸(10 μM;48 小时)引起的 c-MYC mRNA 表达下调 [4]。
|
|---|---|
| 体内研究 (In Vivo) |
每天吸入45分钟,持续两周,异维A酸(1.3-481μg/L;也称为13-顺式视黄酸)可以有效预防A/J小鼠的肺癌[2]。在大鼠中,异维A酸可加速拔牙后的肺泡愈合[3]。
|
| 细胞实验 |
细胞活力测定[4]
细胞类型: HepG2 测试浓度: 0.1、0.5、1、5、10、20 和 40 μM 孵育持续时间:24、48、72 和 96 小时 实验结果:证明 96 小时时细胞活力显着降低(小于 30%)所有剂量。 RT-PCR[4] 细胞类型: HepG2 测试浓度: 10 µM 孵育时间: 48 小时 实验结果: c-MYC mRNA 的表达显着降低约 80%。 |
| 动物实验 |
Animal/Disease Models: Male A/J mice, lung carcinogenesis model[2]
Doses: 1.3, 20.7, or 481 μg/L Route of Administration: Inhalation exposure, 45 min daily for 2 weeks Experimental Results: decreased the tumor multiplicity. Caused up-regulation of lung tissue nuclear retinoic acid receptors (RARs) relative to vehicle-exposed mice, RARα (3.9-fold vehicle), RARβ (3.3-fold), and RARγ (3.7-fold) at 20.7 μg/L. Animal/Disease Models: Wistar rats, tooth extraction model[3] Doses: 7.5 mg/kg Route of Administration: po (oral gavage), daily for 30 days Experimental Results: Accelerated the process of alveolar repair, Dramatically diminished serum calcium levels. |
| 药代性质 (ADME/PK) |
Absorption, Distribution and Excretion
Patients reach a maximum concentration of 74-511ng/mL after 1-4 hours following a 100mg oral dose. Isotretinoin is better absorbed with a high fat meal and bioavailability may change from one brand to another. Following a 40mg oral dose, fasted subjects reached a maximum concentration of 314ng/mL in 2.9 hours with an area under the curve of 4055ng/mL\*hr. Subjects given a high fat meal and a 40mg oral doses reached a maximum concentration of 395ng/mL in 6.4 hours with an area under the curve of 6095ng/mL\*mL. Isotretinoin and its metabolites are conjugated and excreted in the urine and feces in similar amounts. 53-74% of an oral dose is eliminated as unchanged isotretinoin in the feces. The volume of distribution in humans is unknown because there is no intravenous preparation. In a study of pediatric patients with neuroblastoma the volume of distribution was found to be 85L. The volume of distribution was also found to be 2432mL/kg in guinea pigs and 1716mL/kg in obese rats. The clearance of isotretinoin is 15.9L/h in pediatric patients with neuroblastoma. Clearance is also 21.3mL/min/kg in guinea pigs and 7.2mL/min/kg in obese rats. Following oral administration of isotretinoin, there is an apparent lag time of about 0.5-2 hours before the drug appears in systemic circulation. The lag time is thought to result from disintegration of the capsule and subsequent dissolution of the drug in GI contents. Absorption of the drug after this lag time is rapid. The actual bioavailability of orally administered isotretinoin has not been determined in humans, but studies in animals indicate that about 25% of an oral dose of the drug reaches systemic circulation as unchanged isotretinoin The low bioavailability observed in animals may result from biodegradation of the drug in the GI lumen and/or metabolism of the drug during absorption (in the GI mucosa) and first pass through the liver. Food and/or milk increase GI absorption of isotretinoin. Peak blood isotretinoin concentrations are slightly delayed and substantially increased and the area under the blood concentration-time curve (AUC) of the drug is approximately 1.5-2 times greater when isotretinoin is administered 1 hour before, concomitantly with, or 1 hour after a meal than when the drug is administered in the fasting state. Because of its high lipophilicity, oral absorption of isotretinoin is enhanced when the drug is administered with a high-fat meal. In a crossover study of 74 healthy adults who received a single 80-mg isotretinoin dose (as two 40-mg capsules) under fasted and fed conditions, both the peak plasma concentration and total area under the plasma concentration-time curve (AUC) of the drug were more than doubled when isotretinoin was administered immediately after a standardized high-fat meal compared with administration in the fasted state. Because the observed elimination half-life of the drug remained unchanged, it is suggested that food appears to increase the bioavailability of isotretinoin without altering its disposition. The time to peak concentration was also increased with food and may be related to a longer absorption phase. Consequently, the manufacturers recommend that isotretinoin capsules always be administered with food. The harmonic mean elimination for the simultaneous iv and oral administration of isotretinoin was approx 5.5 hr. The mean blood clearance, following iv admin, and the intrinsic clearance, following oral administration, were 5.19 and 6.63 mL/min/kg, respectively. The average abs bioavailability was approx 21% indicating an overall 1st-pass effect of approx 80%. Analysis of gut contents for total (14)-C activity suggested that a fraction of the isotretinoin dose was biologically or chemically degraded in the gut lumen prior to absorption. Clinical doses of isotretinoin range from 0.5 to 8 mg/kg/day, with acute side effects appearing following doses of 1 mg/kg/day or greater. Plasma concn of isotretinoin following single and multiple doses peak between 2 to 4 hr and exhibit elimination half-lives of 10 to 20 hr. Isotretinoin blood concn-time curves following a single- or multiple-dose regimen are well described by a linear model with biphasic disposition characteristics. ... In most conditions, the retinoids produce a maximal effect in about 8 weeks (at the highest tolerated dose), with a slow recurrence of symptoms usually occurring within several weeks following cessation of treatment - except in the treatment of cystic acne with isotretinoin. Maintenance or intermittent dosing usually results in a prolongation of remission. A case study involving the disposition of 13-cis retinoic acid in embryonic tissues from a woman who unintentionally took 40 mg/day of isotretinoin from day 8-28 of gestation was discussed. When the pregnancy was terminated on day 31, between 72 and 80 hr after the last dose of isotretinoin, maternal serum samples were obtained. Retinoid concn in the maternal serum, embryonic tissue, and 6 samples of placental tissue were later measured by high performance liquid chromatography. The results showed that in humans, the intake of isotretinoin during pregnancy results in high placental and embryonic concn of all-trans-retoinic acid, in contrast to what was previously discovered in mice experiments. It was concluded that the metabolic activation of isotretinoin to the all-trans isomer could be responsible for the teratogenicity of isotretinoin. For more Absorption, Distribution and Excretion (Complete) data for 13-cis-Retinoic acid (11 total), please visit the HSDB record page. Metabolism / Metabolites Isotretinoin, or 13-cis-retinoic acid can undergo reversible cis-trans isomerization to all-trans-retinoic acid. Isotretinoin undergoes 4-hydroxylation to 4-hydroxy-13-cis-retinoic acid, which is oxidized to the main metabolite 4-oxo-13-cis-retinoic acid.. All-trans-retinoic acid undergoes 4-hydroxylation to 4-hydroxy-all-trans-retinoic acid, which is oxidized to 4-oxo-all-trans-retinoic acid. 4-oxo-13-cis-retinoic acid can undergo reversible cis-trans isomerization to 4-oxo-all-trans-retinoic acid. ... In human volunteers and patients, one major blood metabolite of isotretinoin is 4-oxo-isotretinoin which undergoes slower elimination than isotretinoin and may itself be a participant in teratogenesis. This paper reviews the teratogenicity of isotretinoin in regard to aspects of species variation, toxicokinetics, and metabolism. The insensitive species (rat, mouse) eliminate the drug rapidly through detoxification to the beta-glucuronide; also, placental transfer is limited in these species. On the other hand, in sensitive species (primates), the drug is predominantly metabolized to the active 13-cis-4-oxo-retinoic acid; placental transfer is more extensive here. The beta-glucuronides showed limited placental transfer in all species examined; these metabolites exhibited very low, if any, measurable concentrations in the human. The 13-cis-retinoic acid is not appreciably bound to cellular retinoid-binding proteins or nuclear receptors and exhibits low tissue distribution and placental transfer. Its access to the nucleus may be extensive. Because of the long half life of 13-cis-retinoic acid, continuous isomerization results in significant area under the concentration-time curve levels of all-trans-retinoic acid in the mouse, monkey and the human; the all-trans-retinoic acid formed is extensively distributed across the placenta and may be an important factor that contributes to the teratogenic potency of 13-cis-retinoic acid. Isomerization cannot explain the teratogenic effects of 13-cis-retinoic acid in the rat and rabbit. It is concluded that the high teratogenic activity of isotretinoin in sensitive species (human, monkey) is related to slow elimination of the 13-cis-isomer, to metabolism to the 4-oxo-derivative, to increased placental transfer, to continuous isomerization and significant exposure of the target tissue to all-trans-retinoic acid; and to lack of binding to cytoplasmic retinoid binding proteins that could possibly result in ready access to the nucleus. Isotretinoin is metabolized in the liver by the cytochrome P-450 (CYP) microsomal enzyme system, principally by CYP2C8, CYP2C9, CYP3A4, and CYP2B6 isoenzymes, to several metabolites (e.g., 4-oxo-isotretinoin, retinoic acid [tretinoin], and 4-oxo-retinoic acid [4-oxo-tretinoin]). Retinoic acid and 13-cis-retinoic acid are geometric isomers and show reversible interconversion, and the administration of one isomer will give rise to the other. Isotretinoin also is irreversibly oxidized to 4-oxo-isotretinoin, which forms its own geometric isomer, 4-oxo-tretinon. All of these metabolites possess retinoid activity that is more than that of the parent compound in some in vitro models. However, the clinical importance of these models is unknown. Concurrent administration of food has been shown to increase the extent of formation of all metabolites in plasma when compared to administration of isotretinoin under fasted conditions. In addition, the exposure of patients to 4-oxo-isotretinoin at steady-state under fasted and fed conditions was approximately 3.4 times higher than that of isotretinoin. In vitro studies indicate that the primary P450 isoforms involved in isotretinoin metabolism are 2C8, 2C9, 3A4 and 2B6. Isotretinoin and its metabolites are further metabolized into conjugates, which are then excreted in urine and feces. For more Metabolism/Metabolites (Complete) data for 13-cis-Retinoic acid (6 total), please visit the HSDB record page. Isotretinoin has known human metabolites that include (2Z,4E,6Z,8E)-6-hydroxy-3,7-dimethyl-9-(2,6,6-trimethylcyclohexen-1-yl)nona-2,4,6,8-tetraenoic acid. Biological Half-Life The half life ranges from 7-39 hours with a mean elimination half life of 20 hours. The half life of 4-oxo-13-cis-retinoic acid ranges from 17-50 hours with a mean elimination half life of 25 hours. Following oral administration of an 80 mg dose of (14)C-isotretinoin as a liquid suspension, (14)C-activity in blood declined with a half-life of 90 hours. After a single 80 mg oral dose of isotretinoin to 74 healthy adult subjects under fed conditions, the mean +/- SD elimination half-lives of isotretinoin and 4-oxo-isotretinoin were 21 +/- 8.2 hours and 24 +/- 5.3 hours, respectively. Blood concentrations of isotretinoin decline in a biphasic manner. In adults with normal renal function, the half-life in the initial phase averages 0.5 hours and the half-life in the terminal phase averages 10-20 hours (range: 7-39 hours). ... Plasma concentration of isotretinoin following single and multiple doses peak between 2 to 4 hr and exhibit elimination half-lives of 10 to 20 hr ... For more Biological Half-Life (Complete) data for 13-cis-Retinoic acid (6 total), please visit the HSDB record page. |
| 毒性/毒理 (Toxicokinetics/TK) |
Hepatotoxicity
Liver test abnormalities occur in up to 15% of patients on isotretinoin, although marked elevations above three times the upper limit of normal or requiring drug discontinuation are rare ( Likelihood score: D (possible rare cause of clinically apparent liver injury). Effects During Pregnancy and Lactation ◉ Summary of Use during Lactation No information is available on the use of isotretinoin during breastfeeding. Various topical agents that are less likely to be absorbed by the mother may be preferred during breastfeeding, especially while nursing a newborn or preterm infant. ◉ Effects in Breastfed Infants Relevant published information was not found as of the revision date. ◉ Effects on Lactation and Breastmilk A woman who had weaned her infant 18 months previously developed a nipple discharge from her right breast after 5.5 months of therapy with isotretinoin. Microbiological, hormonal (including prolactin), radiologic, and physical examinations were otherwise normal. One month after discontinuing isotretinoin, the discharge ceased. After isotretinoin was reinstituted at the same dose, the discharge reappeared within 10 days.[1] The galactorrhea was probably caused by isotretinoin. A review of adverse reaction reports on retinoids causing a breast reaction submitted to a French pharmacovigilance center found 22 cases of gynecomastia was associated with isotretinoin use. Fourteen of the cases were gynecomastia, 6 were galactorrhea and 2 were of both gynecomastia and galactorrhea. Gynecomastia and/or galactorrhea was unilateral for almost half of the reported retinoid cases. The median time of onset was 90 days (IQR 39 to 347 days). The outcome was known for 27 of 31 patients and a total recovery after withdrawal of retinoid was observed for 63% of them.[2] ◈ What is isotretinoin? Isotretinoin is a prescription medication taken by mouth (orally) to treat severe cystic acne when other treatments have not worked. Isotretinoin is a form of Vitamin A. It has been sold under brand names such as Accutane®, Absorica®, Amnesteem®, Claravis®, Epuris®, Clarus®, Myorisan®, Sotret®, and Zenatane®.The product label for isotretinoin recommends people who are pregnant do not use this medication. This is because using isotretinoin in pregnancy can lead to birth defects and other pregnancy related problems. If you are taking isotretinoin and find out you are pregnant, stop taking the medication and contact your healthcare provider right away. If you are taking isotretinoin and want to get pregnant, talk with your healthcare provider about your condition and what treatment is best for you. ◈ I take isotretinoin. Can it make it harder for me to get pregnant? People who are trying to get pregnant should not be taking isotretinoin. There have been reports of changes in the menstrual cycle (periods) in some people taking isotretinoin. There are no reports of problems getting pregnant while taking isotretinoin. ◈ I am taking isotretinoin, but I would like to stop taking it before pregnancy. How long does it stay in my body? People eliminate medication at different rates. In healthy adults, it takes up to 6 days, on average, for most of the isotretinoin to be gone from the body. However, it is recommended that a person wait one month after stopping isotretinoin before trying to get pregnant. ◈ I just found out I am pregnant. Should I stop taking isotretinoin? Yes, it is recommended that you stop taking isotretinoin right away if you find out you are pregnant. As soon as possible, call the healthcare provider who prescribed the isotretinoin and the healthcare provider who will be taking care of you during your pregnancy. Isotretinoin can cause birth defects. Your healthcare team can talk with you about the risks to your pregnancy and available options. ◈ Does taking isotretinoin increase the chance of miscarriage? Miscarriage is common and can occur in any pregnancy for many different reasons. Taking isotretinoin can increase the chance of miscarriage. The chance of having a miscarriage can be as high as 40% when isotretinoin is used in early pregnancy. ◈ Does taking isotretinoin increase the chance of birth defects? Every pregnancy starts out with a 3-5% chance of having a birth defect. This is called the background risk. Isotretinoin causes birth defects in up to 35% or more of infants who are exposed during pregnancy. There is a chance of having a baby with a birth defect even if the medication has been taken for a short time. Most of the infants with birth defects will have small or absent ears and hearing and eyesight problems. Other issues that have also been reported include: heart defects, fluid around the brain, small jaw, small head, cleft palate (opening in the roof of the mouth), and being born with a small or missing thymus gland (a gland that makes hormones). While not every pregnancy exposed to isotretinoin will have birth defects, it is recommended to avoid any isotretinoin use in pregnancy. ◈ Does taking isotretinoin in pregnancy increase the chance of other pregnancy-related problems? An increased chance for preterm delivery (birth before week 37) has been associated with the use of isotretinoin in pregnancy. ◈ Does taking isotretinoin in pregnancy affect future behavior or learning for the child? Children exposed to isotretinoin during pregnancy can have hearing and eyesight problems, which can cause issues with learning. Exposed children can also have moderate to severe behavioral problems and/or intellectual disability. These issues are not usually noticed at birth but are found later as the child grows. Other possible long-term effects on children exposed to isotretinoin during pregnancy are unknown. ◈ What screenings or tests are available to see if my pregnancy has birth defects or other issues? Prenatal ultrasounds can be used to screen for some birth defects. Ultrasound can also be used to monitor the growth of the pregnancy. Talk with your healthcare provider about any prenatal screenings or testing that are available to you. There are no tests available during pregnancy that can tell how much effect there could be on future behavior or learning. ◈ Can I still get a prescription for isotretinoin? Isotretinoin can be prescribed under a special program called iPLEDGE® Risk Evaluation and Mitigation Strategy (REMS). People MUST adhere to all requirements of the program to get prescriptions for isotretinoin. The following are some of the requirements:Must talk with your healthcare provider about isotretinoin and the iPLEDGE® REMS program.Must be able to understand that severe birth defects can occur with use of isotretinoin.Must receive and be able to understand safety information about isotretinoin and the iPLEDGE® REMS program requirements.Must be enrolled by your healthcare provider in the iPLEDGE® REMS program for 30 days before first prescription.Must read, understand, and sign an informed consent form that contains warnings about the risks of using isotretinoin.Must correctly answer comprehensive questions in the iPLEDGE® REMS program website.Must not be pregnant, trying to get pregnant, or breastfeeding.Must have two (2) negative pregnancy tests before starting isotretinoin.Must have a pregnancy test every month during treatment.Must have a negative pregnancy test before each monthly prescription.Must use two (2) different forms of birth control at all times (unless agrees not to have sex) starting one (1) month before treatment, continue using 2 forms during treatment, and also for one (1) month after treatment.Must fill prescription within 7 days after the health care provider visit.Must agree to see your healthcare provider every month during treatment for a health check and to get a new prescription.Must not share medication with anyone.Must not donate blood during treatment and for one (1) month after treatment.For more information about the iPLEDGE program call 1-866-495-0654 or visit the iPLEDGE website at https://www.ipledgeprogram.com.Even if you are not sexually active or planning a pregnancy, if you use or want to use isotretinoin it is recommended that you talk to your healthcare provider. Using effective birth control methods is important because almost 50% of all pregnancies are unplanned or unintended. ◈ Breastfeeding while taking isotretinoin: The product label for isotretinoin recommends people who are breastfeeding not use this medication. There have been no studies looking at the use of isotretinoin during breastfeeding. It is not known what effect, if any, exposure to isotretinoin through breast milk can have on a nursing infant. Be sure to talk to your healthcare provider about all your breastfeeding questions. ◈ If a male takes isotretinoin, could it affect fertility or increase the chance of birth defects? There have been a few reports of erectile dysfunction (trouble with getting and keeping an erection) and ejaculatory failure (no seminal fluid comes out of the penis) in males taking isotretinoin. This can affect fertility (ability to get partner pregnant). Studies have not been done in males to see if isotretinoin could increase the chance of birth defects. In general, exposures that fathers or sperm donors have are unlikely to increase risks to a pregnancy. For more information, please see the MotherToBaby fact sheet Paternal Exposures at https://mothertobaby.org/fact-sheets/paternal-exposures-pregnancy/. Protein Binding Isotretinoin is >99.9% protein bound, mainly to serum albumin. |
| 参考文献 |
[1]. Layton A. The use of isotretinoin in acne. Dermatoendocrinol. 2009 May;1(3):162-9.
[2]. Dahl AR, et al. Inhaled isotretinoin (13-cis retinoic acid) is an effective lung cancer chemopreventive agent in A/J mice at low doses: a pilot study. Clin Cancer Res. 2000 Aug;6(8):3015-24 [3]. Bergoli RD, et al. Isotretinoin effect on alveolar repair after exodontia--a study in rats. Oral Maxillofac Surg. 2011 Jun;15(2):85-92. [4]. Ramírez-Flores PN, et al. Isotretinoin and Thalidomide Down-Regulate c-MYC Gene Expression and Modify Proteins Associated with Cancer in Hepatic Cells. Molecules. 2021 Sep 22;26(19):5742. |
| 其他信息 |
Isotretinoin can cause developmental toxicity according to an independent committee of scientific and health experts.
Cis-retinoic acid is a yellow-orange to orange crystalline powder; orange-brown chunky solid. (NTP, 1992) Isotretinoin is a retinoic acid that is all-trans-retinoic acid in which the double bond which is alpha,beta- to the carboxy group is isomerised to Z configuration. A synthetic retinoid, it is used for the treatment of severe cases of acne and other skin diseases. It has a role as a keratolytic drug, an antineoplastic agent and a teratogenic agent. It is a conjugate acid of a 13-cis-retinoate. Isotretinoin is a retinoid derivative of vitamin A used in the treatment of severe recalcitrant acne. It was most widely marketed under the brand name Accutane, which has since been discontinued. Isotretinoin is associated with major risks in pregnancy and is therefore only available under the iPLEDGE program in the United States. The first isotretinoin-containing product was FDA approved on 7 May 1982. Isotretinoin is a Retinoid. Isotretinoin is a retinoid and vitamin A derivative used in the treatment of severe acne and some forms of skin, head and neck cancer. Isotretinoin, like many retinoids, can lead to increase in serum aminotransferase levels, but, unlike acitretin and etretinate, isotretinoin has not been clearly implicated in cases of clinically apparent acute liver injury with jaundice. Isotretinoin has been reported in Homo sapiens with data available. Isotretinoin is a naturally-occurring retinoic acid with potential antineoplastic activity. Isotretinoin binds to and activates nuclear retinoic acid receptors (RARs); activated RARs serve as transcription factors that promote cell differentiation and apoptosis. This agent also exhibits immunomodulatory and anti-inflammatory responses and inhibits ornithine decarboxylase, thereby decreasing polyamine synthesis and keratinization. A topical dermatologic agent that is used in the treatment of ACNE VULGARIS and several other skin diseases. The drug has teratogenic and other adverse effects. See also: Isotretinoin Anisatil (is active moiety of). Drug Indication Isotretinoin is indicated to treat severe recalcitrant nodular acne and patients ≥12 years enrolled in the iPLEDGE program. FDA Label Mechanism of Action Isotretinoin produces its effects through altering progress through the cell cycle, cell differentiation, survival, and apoptosis. These actions reduce sebum production, preventing the blockage of pores, and growth of acne causing bacteria. Isotretinoin and 4-oxo-isotretinoin both significantly reduce the production of sebum. Isotretinoin has little to no affinity for retinol binding proteins (RBPs) and retinoic acid nuclear receptors (RARs). Tretinoin and 4-oxo-tretinion bind to the RAR-γ receptor, which is suspected to be part of the action of acne treatment by isotretinoin. Isotretinoin induces apoptosis in sebocytes, leading to a decrease in sebum production. Isotretinoin also reduces the formation of comedones by reducing hyperkeratinization through an unknown mechanism. Isotretinoin does not directly kill bacteria but it does reduce the size of sebum ducts and makes the microenvironment less hospitable to acne causing bacteria. It may also increase immune mechanisms and alter chemotaxis of monocytes to reduce inflammation. There is preliminary evidence suggesting isotretinoin may interact with FoxO1, which may explain a substantial number of isotretinoin's unexplained actions. This paper reviews the teratogenicity of isotretinoin in regard to aspects of species variation, toxicokinetics, and metabolism. The insensitive species (rat, mouse) eliminate the drug rapidly through detoxification to the beta-glucuronide; also, placental transfer is limited in these species. On the other hand, in sensitive species (primates), the drug is predominantly metabolized to the active 13-cis-4-oxo-retinoic acid; placental transfer is more extensive here. The beta-glucuronides showed limited placental transfer in all species examined; these metabolites exhibited very low, if any, measurable concentrations in the human. The 13-cis-retinoic acid is not appreciably bound to cellular retinoid-binding proteins or nuclear receptors and exhibits low tissue distribution and placental transfer. Its access to the nucleus may be extensive. Because of the long half life of 13-cis-retinoic acid, continuous isomerization results in significant area under the concentration-time curve levels of all-trans-retinoic acid in the mouse, monkey and the human; the all-trans-retinoic acid formed is extensively distributed across the placenta and may be an important factor that contributes to the teratogenic potency of 13-cis-retinoic acid. Isomerization cannot explain the teratogenic effects of 13-cis-retinoic acid in the rat and rabbit. It is concluded that the high teratogenic activity of isotretinoin in sensitive species (human, monkey) is related to slow elimination of the 13-cis-isomer, to metabolism to the 4-oxo-derivative, to increased placental transfer, to continuous isomerization and significant exposure of the target tissue to all-trans-retinoic acid; and to lack of binding to cytoplasmic retinoid binding proteins that could possibly result in ready access to the nucleus. |
| 分子式 |
C20H28O2
|
|
|---|---|---|
| 分子量 |
300.44
|
|
| 精确质量 |
300.208
|
|
| CAS号 |
4759-48-2
|
|
| 相关CAS号 |
Isotretinoin-d5
|
|
| PubChem CID |
5282379
|
|
| 外观&性状 |
Yellow crystals or reddish-orange plates from isopropyl alcohol
Yellowish to orange crystalline powder |
|
| 密度 |
1.0±0.1 g/cm3
|
|
| 沸点 |
462.8±14.0 °C at 760 mmHg
|
|
| 熔点 |
172-175 °C(lit.)
|
|
| 闪点 |
350.6±11.0 °C
|
|
| 蒸汽压 |
0.0±2.5 mmHg at 25°C
|
|
| 折射率 |
1.556
|
|
| LogP |
6.83
|
|
| tPSA |
37.3
|
|
| 氢键供体(HBD)数目 |
1
|
|
| 氢键受体(HBA)数目 |
2
|
|
| 可旋转键数目(RBC) |
5
|
|
| 重原子数目 |
22
|
|
| 分子复杂度/Complexity |
567
|
|
| 定义原子立体中心数目 |
0
|
|
| SMILES |
CC1(C)C(/C=C/C(C)=C/C=C/C(C)=C\C(O)=O)=C(C)CCC1
|
|
| InChi Key |
SHGAZHPCJJPHSC-XFYACQKRSA-N
|
|
| InChi Code |
InChI=1S/C20H28O2/c1-15(8-6-9-16(2)14-19(21)22)11-12-18-17(3)10-7-13-20(18,4)5/h6,8-9,11-12,14H,7,10,13H2,1-5H3,(H,21,22)/b9-6+,12-11+,15-8+,16-14-
|
|
| 化学名 |
(2Z,4E,6E,8E)-3,7-dimethyl-9-(2,6,6-trimethylcyclohex-1-en-1-yl)nona-2,4,6,8-tetraenoic acid
|
|
| 别名 |
|
|
| HS Tariff Code |
2934.99.9001
|
|
| 存储方式 |
Powder -20°C 3 years 4°C 2 years In solvent -80°C 6 months -20°C 1 month 注意: (1). 本产品在运输和储存过程中需避光。 (2). 请将本产品存放在密封且受保护的环境中(例如氮气保护),避免吸湿/受潮。 (3). 该产品在溶液状态不稳定,请现配现用。 |
|
| 运输条件 |
Room temperature (This product is stable at ambient temperature for a few days during ordinary shipping and time spent in Customs)
|
| 溶解度 (体外实验) |
|
|||
|---|---|---|---|---|
| 溶解度 (体内实验) |
配方 1 中的溶解度: ≥ 2.5 mg/mL (8.32 mM) (饱和度未知) in 10% DMSO + 40% PEG300 + 5% Tween80 + 45% Saline (这些助溶剂从左到右依次添加,逐一添加), 澄清溶液。
例如,若需制备1 mL的工作液,可将100 μL 25.0 mg/mL澄清DMSO储备液加入到400 μL PEG300中,混匀;然后向上述溶液中加入50 μL Tween-80,混匀;加入450 μL生理盐水定容至1 mL。 *生理盐水的制备:将 0.9 g 氯化钠溶解在 100 mL ddH₂O中,得到澄清溶液。 配方 2 中的溶解度: ≥ 2.08 mg/mL (6.92 mM) (饱和度未知) in 10% DMSO + 90% Corn Oil (这些助溶剂从左到右依次添加,逐一添加), 澄清溶液。 例如,若需制备1 mL的工作液,可将 100 μL 20.8 mg/mL 澄清 DMSO 储备液加入到 900 μL 玉米油中并混合均匀。 请根据您的实验动物和给药方式选择适当的溶解配方/方案: 1、请先配制澄清的储备液(如:用DMSO配置50 或 100 mg/mL母液(储备液)); 2、取适量母液,按从左到右的顺序依次添加助溶剂,澄清后再加入下一助溶剂。以 下列配方为例说明 (注意此配方只用于说明,并不一定代表此产品 的实际溶解配方): 10% DMSO → 40% PEG300 → 5% Tween-80 → 45% ddH2O (或 saline); 假设最终工作液的体积为 1 mL, 浓度为5 mg/mL: 取 100 μL 50 mg/mL 的澄清 DMSO 储备液加到 400 μL PEG300 中,混合均匀/澄清;向上述体系中加入50 μL Tween-80,混合均匀/澄清;然后继续加入450 μL ddH2O (或 saline)定容至 1 mL; 3、溶剂前显示的百分比是指该溶剂在最终溶液/工作液中的体积所占比例; 4、 如产品在配制过程中出现沉淀/析出,可通过加热(≤50℃)或超声的方式助溶; 5、为保证最佳实验结果,工作液请现配现用! 6、如不确定怎么将母液配置成体内动物实验的工作液,请查看说明书或联系我们; 7、 以上所有助溶剂都可在 Invivochem.cn网站购买。 |
| 制备储备液 | 1 mg | 5 mg | 10 mg | |
| 1 mM | 3.3285 mL | 16.6423 mL | 33.2845 mL | |
| 5 mM | 0.6657 mL | 3.3285 mL | 6.6569 mL | |
| 10 mM | 0.3328 mL | 1.6642 mL | 3.3285 mL |
1、根据实验需要选择合适的溶剂配制储备液 (母液):对于大多数产品,InvivoChem推荐用DMSO配置母液 (比如:5、10、20mM或者10、20、50 mg/mL浓度),个别水溶性高的产品可直接溶于水。产品在DMSO 、水或其他溶剂中的具体溶解度详见上”溶解度 (体外)”部分;
2、如果您找不到您想要的溶解度信息,或者很难将产品溶解在溶液中,请联系我们;
3、建议使用下列计算器进行相关计算(摩尔浓度计算器、稀释计算器、分子量计算器、重组计算器等);
4、母液配好之后,将其分装到常规用量,并储存在-20°C或-80°C,尽量减少反复冻融循环。
计算结果:
工作液浓度: mg/mL;
DMSO母液配制方法: mg 药物溶于 μL DMSO溶液(母液浓度 mg/mL)。如该浓度超过该批次药物DMSO溶解度,请首先与我们联系。
体内配方配制方法:取 μL DMSO母液,加入 μL PEG300,混匀澄清后加入μL Tween 80,混匀澄清后加入 μL ddH2O,混匀澄清。
(1) 请确保溶液澄清之后,再加入下一种溶剂 (助溶剂) 。可利用涡旋、超声或水浴加热等方法助溶;
(2) 一定要按顺序加入溶剂 (助溶剂) 。
| NCT Number | Recruitment | interventions | Conditions | Sponsor/Collaborators | Start Date | Phases |
| NCT04660916 | Completed | Drug: Isotretinoin | Isotretinoin Nail Abnormality |
Sinan Özçelik | October 22, 2019 | |
| NCT06225570 | Not yet recruiting | Drug: Isotretinoin Drug: Tetracycline |
Acne Vulgaris | Medical University of South Carolina | February 2024 | Early Phase 1 |
| NCT04204304 | Completed | Drug: Isotretinoin | Isotretinoin Adverse Reaction Vitamin D Deficiency |
Ankara Training and Research Hospital | March 15, 2019 | Not Applicable |
| NCT05218486 | Active, not recruiting | Drug: Isotretinoin | Acne Vulgaris | Alshimaa Abbas Mohamed Ebrahim | August 1, 2021 | Phase 4 |
|
|
|
InvivoChem的所有产品仅用于作科学研究,不面向患者销售
Copyright 2020 InvivoChem LLC | All Rights Reserved 粤ICP备20063088号-1





























 NMR
NMR