| 规格 | 价格 | |
|---|---|---|
| Other Sizes |

| 体外研究 (In Vitro) |
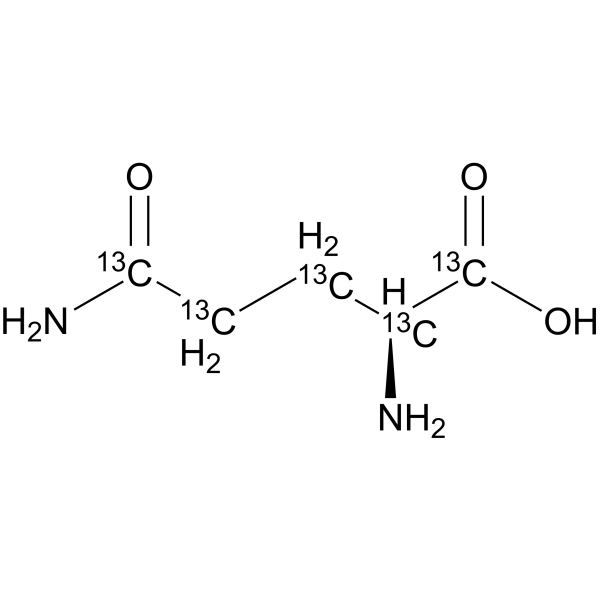
药物化合物经过修饰,加入了氢、碳和其他元素的稳定重同位素。这些同位素主要在药物开发过程中用作定量示踪剂。 1]。
|
|---|---|
| 药代性质 (ADME/PK) |
Absorption, Distribution and Excretion
Absorption is efficient and occurs by an active transport mechanism. Tmax is 30 minutes after a single dose. Absorption kinetics following multiple doses has not yet been determined. Primarily eliminated by metabolism. While L-glutamine is filtered though the glomerulus, nearly all is reabsorbed by renal tubules. Volume of distribution is 200 mL/kg after intravenous bolus dose. After an intravenous bolus dose in three subjects, the volume of distribution was estimated to be approximately 200 mL/kg. Following single dose oral administration of glutamine at 0.1 g/kg to six subjects, mean peak blood glutamine concentration was 1028uM (or 150 mcg/mL) occurring approximately 30 minutes after administration. The pharmacokinetics following multiple oral doses have not been adequately characterized. Metabolism is the major route of elimination for glutamine. Although glutamine is eliminated by glomerular filtration, it is almost completely reabsorbed by the renal tubules. Metabolism / Metabolites Exogenous L-glutamine likely follows the same metabolic pathways as endogenous L-glutamine which is involved in the formation of glutamate, proteins, nucleotides, and amino acid sugars. Glutamine plays an important role in nitrogen homeostasis and intestinal substrate supply. It has been suggested that glutamine is a precursor for arginine through an intestinal-renal pathway involving inter-organ transport of citrulline. The importance of intestinal glutamine metabolism for endogenous arginine synthesis in humans, however, has remained unaddressed. The aim of this study was to investigate the intestinal conversion of glutamine to citrulline and the effect of the liver on splanchnic citrulline metabolism in humans. Eight patients undergoing upper gastrointestinal surgery received a primed continuous intravenous infusion of [2-(15)N]glutamine and [ureido-(13)C-(2)H(2)]citrulline. Arterial, portal venous and hepatic venous blood were sampled and portal and hepatic blood flows were measured. Organ specific amino acid uptake (disposal), production and net balance, as well as whole body rates of plasma appearance were calculated according to established methods. The intestines consumed glutamine at a rate that was dependent on glutamine supply. Approximately 13% of glutamine taken up by the intestines was converted to citrulline. Quantitatively glutamine was the only important precursor for intestinal citrulline release. Both glutamine and citrulline were consumed and produced by the liver, but net hepatic flux of both amino acids was not significantly different from zero. Plasma glutamine was the precursor of 80% of plasma citrulline and plasma citrulline in turn was the precursor of 10% of plasma arginine. In conclusion, glutamine is an important precursor for the synthesis of arginine after intestinal conversion to citrulline in humans. Endogenous glutamine participates in various metabolic activities, including the formation of glutamate, and synthesis of proteins, nucleotides, and amino sugars. Exogenous glutamine is anticipated to undergo similar metabolism. Enterocytes, Hepatic Biological Half-Life The half life of elimination is 1 h. After an IV bolus dose in three subjects, the terminal half-life of glutamine was approximately 1 hour. |
| 毒性/毒理 (Toxicokinetics/TK) |
Toxicity Summary
Supplemental L-glutamine's possible immunomodulatory role may be accounted for in a number of ways. L-glutamine appears to play a major role in protecting the integrity of the gastrointestinal tract and, in particular, the large intestine. During catabolic states, the integrity of the intestinal mucosa may be compromised with consequent increased intestinal permeability and translocation of Gram-negative bacteria from the large intestine into the body. The demand for L-glutamine by the intestine, as well as by cells such as lymphocytes, appears to be much greater than that supplied by skeletal muscle, the major storage tissue for L-glutamine. L-glutamine is the preferred respiratory fuel for enterocytes, colonocytes and lymphocytes. Therefore, supplying supplemental L-glutamine under these conditions may do a number of things. For one, it may reverse the catabolic state by sparing skeletal muscle L-glutamine. It also may inhibit translocation of Gram-negative bacteria from the large intestine. L-glutamine helps maintain secretory IgA, which functions primarily by preventing the attachment of bacteria to mucosal cells. L-glutamine appears to be required to support the proliferation of mitogen-stimulated lymphocytes, as well as the production of interleukin-2 (IL-2) and interferon-gamma (IFN-gamma). It is also required for the maintenance of lymphokine-activated killer cells (LAK). L-glutamine can enhance phagocytosis by neutrophils and monocytes. It can lead to an increased synthesis of glutathione in the intestine, which may also play a role in maintaining the integrity of the intestinal mucosa by ameliorating oxidative stress. The exact mechanism of the possible immunomodulatory action of supplemental L-glutamine, however, remains unclear. It is conceivable that the major effect of L-glutamine occurs at the level of the intestine. Perhaps enteral L-glutamine acts directly on intestine-associated lymphoid tissue and stimulates overall immune function by that mechanism, without passing beyond the splanchnic bed. Hepatotoxicity In clinical trials of L-glutamine in patients with sickle cell disease, serum aminotransferase elevations were not mentioned, and there were no reports of clinically apparent liver injury. Patients with sickle cell disease frequently have jaundice, largely due to chronic hemolysis which raises serum indirect bilirubin levels. They also can have fluctuating liver test abnormalities due to complications of sickle cell disease, such as gall stone disease (from chronic hemolysis), viral hepatitis and iron overload (from blood transfusions), congestive liver disease (due to pulmonary hypertension), and veno-occlusive crises involving the liver which can be associated with serum aminotransferase elevations and hepatic dysfunction. In preregistration trials of L-glutamine, hepatic events were not reported and serious adverse events were no more common with the active drug than with placebo. L-glutamine is a normal constituent of virtually all tissues and is unlikely to have intrinsic toxicity, even in high doses. Glutamine supplementation has a potential of worsening hepatic encephalopathy in patients with advanced cirrhosis. Glutamine is metabolized to glutamate and ammonia which can overwhelm the hepatic elimination of ammonia in patients with severe liver dysfunction. Ingestion of 10 to 20 grams of glutamine has been shown to cause elevations of serum ammonia levels and to worsen psychometric measures of hepatic encephalopathy in patients with decompensated cirrhosis. Plasma ammonia levels do not increase with glutamine supplementation in patients with normal hepatic function, and its effects in patients with cirrhosis is not due to hepatic injury. Nevertheless, use of L-glutamine should be avoided in patients with sickle cell disease and advanced cirrhosis. Likelihood score: E (unlikely cause of acute liver injury with jaundice). Interactions Radiotherapy is often used to treat prostate tumors, but the normal bladder is usually adversely affected. Using an animal model of pelvic radiation, /the authors/ investigated whether glutamine nutritional supplementation can prevent radiation-induced damage to the bladder, especially in its more superficial layers. Male rats aged 3-4 months were divided into groups of 8 animals each: controls, which consisted intact animals; radiated-only rats, which were sacrificed 7 (R7) or 15 (R15) days after a radiation session (10Gy aimed at the pelvico-abdominal region); and radiated rats receiving l-glutamine supplementation (0.65g/kg body weight/day), which were sacrificed 7 (RG7) or 15 (RG15) days after the radiation session. Cells and blood vessels in the vesical lamina propria, as well as the urothelium, were then measured using histological methods. The effects of radiation were evaluated by comparing controls vs. either R7 or R15, while a protective effect of glutamine was assessed by comparing R7 vs. RG7 and R15 vs. RG15. The results showed that, in R7, epithelial thickness, epithelial cell density, and cell density in the lamina propria were not significantly affected. However, density of blood vessels in R7 was reduced by 48% (p<0.05) and this alteration was mostly prevented by glutamine (p<0.02). In R15, density of blood vessels in the lamina propria was not significantly modified. However, epithelial thickness was reduced by 25% (p<0.05) in R15, and this effect was prevented by glutamine (p<0.01). In R15, epithelial cell density was increased by 35% (p<0.02), but glutamine did not protect against this radiation-induced increase. Cell density in the lamina propria was likewise unaffected in R15. Density of mast cells in the lamina propria was markedly reduced in R7 and R15. The density was still reduced in RG7, but a higher density in RG15 suggested a glutamine-mediated recovery. Alpha-actin positive cells in the lamina propria formed a suburothelial layer and were identified as myofibroblasts. Thickness of this layer was increased in R7, but was similar to controls in RG7, while changes in R15 and RG15 were less evident. In conclusion, pelvic radiation leads to significant acute and post-acute alterations in the composition and structural features of the vesical lamina propria and epithelium. Most of these changes, however, can be prevented by glutamine nutritional supplementation. These results emphasize, therefore, the potential use of this aminoacid as a radioprotective drug. Glutamine is a neutral amino acid that is used by rapidly dividing cells such as erythrocytes, lymphocytes, and fibroblasts. It is also the substrate of glutathione synthesis. In normal metabolic rates, glutamine is an amino acid synthesized endogenously, but in high metabolic conditions such as cancer, it must be taken exogenously. Animal studies strongly demonstrate that glutamine protects both the upper and lower gastrointestinal tract mucosa from the effects of chemotherapy, radiotherapy, or other causes of injury. In this study, ... the protective effect of glutamine on radiation-induced diarrhea /was investigated/.The patients were divided into glutamine-treated and placebo groups. In the glutamine-treated group, 15 g of oral glutamine was administered three times daily. The patients were evaluated for diarrhea grade according to the National Cancer Institute Common Toxicity Criteria version 3.0, need for loperamide use, need for supportive parenteral therapy, and treatment breaks due to diarrhea. There was no difference in overall diarrhea incidence when the two groups were compared. When diarrhea grade was evaluated, none of the patients in the glutamine-treated group had grade 3-4 diarrhea, but in the placebo group, grade 3-4 diarrhea was seen in 69% of the patients. In the placebo-treated group, patients requiring loperamide and parenteral supportive therapy were 39 and 92 %, respectively. There was no treatment break in glutamine-treated patients. Glutamine may have protective effect on radiation-induced severe diarrhea. Non-Human Toxicity Values LD50 Mouse oral 700 mg/kg LD50 Rat oral 7500 mg/kg |
| 参考文献 |
|
| 其他信息 |
Therapeutic Uses
EXPL THER Glutamine depletion has negative effects on the functional integrity of the gut and leads to immunosuppression. Very low birth weight (VLBW) infants are susceptible to glutamine depletion, as enteral nutrition is limited in the first weeks of life. Enteral glutamine supplementation may have a positive effect on feeding tolerance, infectious morbidity and short-term outcome. The aim of the study was to determine the effect of enteral glutamine supplementation on plasma amino acid concentrations, reflecting one aspect of safety of enteral glutamine supplementation in VLBW infants. In a double-blind placebo-controlled randomized controlled trial, VLBW infants (gestational age <32 weeks or birth weight <1500 g) received enteral glutamine supplementation (0.3 g/kg per day) or isonitrogenous placebo supplementation (alanine) between day 3 and day 30 of life. Supplementation was added to breast milk or to preterm formula. Plasma amino acid concentrations were measured at four time points: before the start of the study and at days 7, 14 and 30 of life.Baseline patient and nutritional characteristics were not different in glutamine (n = 52) and control (n = 50) groups. Plasma concentrations of most essential and non-essential amino acids increased throughout the study period. There was no effect of enteral glutamine supplementation. In particular, the increase of plasma glutamine and glutamate concentrations was not different between the treatment groups (P = 0.49 and P = 0.34 respectively, day 30).Enteral glutamine supplementation in VLBW infants does not alter plasma concentrations of glutamine, glutamate or other amino acids. Enteral supplementation in a dose of 0.3 g/kg per day seems safe in VLBW infants. EXPL THER Critically ill patients have considerable oxidative stress. Glutamine and antioxidant supplementation may offer therapeutic benefit, although current data are conflicting.In this blinded 2-by-2 factorial trial, we randomly assigned 1223 critically ill adults in 40 intensive care units (ICUs) in Canada, the United States, and Europe who had multiorgan failure and were receiving mechanical ventilation to receive supplements of glutamine, antioxidants, both, or placebo. Supplements were started within 24 hours after admission to the ICU and were provided both intravenously and enterally. The primary outcome was 28-day mortality. Because of the interim-analysis plan, a P value of less than 0.044 at the final analysis was considered to indicate statistical significance. There was a trend toward increased mortality at 28 days among patients who received glutamine as compared with those who did not receive glutamine (32.4% vs. 27.2%; adjusted odds ratio, 1.28; 95% confidence interval [CI], 1.00 to 1.64; P=0.05). In-hospital mortality and mortality at 6 months were significantly higher among those who received glutamine than among those who did not. Glutamine had no effect on rates of organ failure or infectious complications. Antioxidants had no effect on 28-day mortality (30.8%, vs. 28.8% with no antioxidants; adjusted odds ratio, 1.09; 95% CI, 0.86 to 1.40; P=0.48) or any other secondary end point. There were no differences among the groups with respect to serious adverse events (P=0.83). Early provision of glutamine or antioxidants did not improve clinical outcomes, and glutamine was associated with an increase in mortality among critically ill patients with multiorgan failure. NutreStore (L-glutamine powder for oral solution) is indicated for the treatment of Short Bowel Syndrome (SBS) in patients receiving specialized nutritional support when used in conjunction with a recombinant human growth hormone that is approved for this indication. /Included in US product label/ Drug Warnings The safety and effectiveness of L-glutamine in pediatric patients have not been established. It is not known whether L-glutamine is excreted in human milk. Because many drugs are excreted in human milk, caution should be exercised when L-glutamine is administered to a nursing woman. Glutamine is metabolized to glutamate and ammonia, which may increase in patients with hepatic dysfunction. Therefore, routine monitoring of renal and hepatic function is recommended in patients receiving intravenous parenteral nutrition (IPN) and NutreStore, particularly in those with renal or hepatic impairment. FDA Pregnancy Risk Category: C /RISK CANNOT BE RULED OUT. Adequate, well controlled human studies are lacking, and animal studies have shown risk to the fetus or are lacking as well. There is a chance of fetal harm if the drug is given during pregnancy; but the potential benefits may outweigh the potential risk./ For more Drug Warnings (Complete) data for Glutamine (7 total), please visit the HSDB record page. Pharmacodynamics Like other amino acids, glutamine is biochemically important as a constituent of proteins. Glutamine is also crucial in nitrogen metabolism. Ammonia (formed by nitrogen fixation) is assimilated into organic compounds by converting glutamic acid to glutamine. The enzyme which accomplishes this is called glutamine synthetase. Glutamine can then be used as a nitrogen donor in the biosynthesis of many compounds, including other amino acids, purines, and pyrimidines. L-glutamine improves nicotinamide adenine dinucleotide (NAD) redox potential. |
| 分子式 |
13C5H10N2O3
|
|---|---|
| 分子量 |
151.11
|
| 精确质量 |
146.069
|
| CAS号 |
184161-19-1
|
| 相关CAS号 |
L-Glutamine;56-85-9
|
| PubChem CID |
5961
|
| 外观&性状 |
White to off-white solid powder
|
| 熔点 |
185°C (dec.) (lit.)
|
| LogP |
0.064
|
| tPSA |
106.41
|
| 氢键供体(HBD)数目 |
3
|
| 氢键受体(HBA)数目 |
4
|
| 可旋转键数目(RBC) |
4
|
| 重原子数目 |
10
|
| 分子复杂度/Complexity |
146
|
| 定义原子立体中心数目 |
1
|
| SMILES |
C(CC(=O)N)[C@@H](C(=O)O)N
|
| InChi Key |
ZDXPYRJPNDTMRX-VKHMYHEASA-N
|
| InChi Code |
InChI=1S/C5H10N2O3/c6-3(5(9)10)1-2-4(7)8/h3H,1-2,6H2,(H2,7,8)(H,9,10)/t3-/m0/s1
|
| 化学名 |
(2S)-2,5-diamino-5-oxopentanoic acid
|
| HS Tariff Code |
2934.99.9001
|
| 存储方式 |
Powder -20°C 3 years 4°C 2 years In solvent -80°C 6 months -20°C 1 month |
| 运输条件 |
Room temperature (This product is stable at ambient temperature for a few days during ordinary shipping and time spent in Customs)
|
| 溶解度 (体外实验) |
H2O : 31.25 mg/mL (206.80 mM)
|
|---|---|
| 溶解度 (体内实验) |
配方 1 中的溶解度: 16.67 mg/mL (110.32 mM) in PBS (这些助溶剂从左到右依次添加,逐一添加), 澄清溶液; 超声助溶。 (<60°C).
请根据您的实验动物和给药方式选择适当的溶解配方/方案: 1、请先配制澄清的储备液(如:用DMSO配置50 或 100 mg/mL母液(储备液)); 2、取适量母液,按从左到右的顺序依次添加助溶剂,澄清后再加入下一助溶剂。以 下列配方为例说明 (注意此配方只用于说明,并不一定代表此产品 的实际溶解配方): 10% DMSO → 40% PEG300 → 5% Tween-80 → 45% ddH2O (或 saline); 假设最终工作液的体积为 1 mL, 浓度为5 mg/mL: 取 100 μL 50 mg/mL 的澄清 DMSO 储备液加到 400 μL PEG300 中,混合均匀/澄清;向上述体系中加入50 μL Tween-80,混合均匀/澄清;然后继续加入450 μL ddH2O (或 saline)定容至 1 mL; 3、溶剂前显示的百分比是指该溶剂在最终溶液/工作液中的体积所占比例; 4、 如产品在配制过程中出现沉淀/析出,可通过加热(≤50℃)或超声的方式助溶; 5、为保证最佳实验结果,工作液请现配现用! 6、如不确定怎么将母液配置成体内动物实验的工作液,请查看说明书或联系我们; 7、 以上所有助溶剂都可在 Invivochem.cn网站购买。 |
| 制备储备液 | 1 mg | 5 mg | 10 mg | |
| 1 mM | 6.6177 mL | 33.0885 mL | 66.1770 mL | |
| 5 mM | 1.3235 mL | 6.6177 mL | 13.2354 mL | |
| 10 mM | 0.6618 mL | 3.3088 mL | 6.6177 mL |
1、根据实验需要选择合适的溶剂配制储备液 (母液):对于大多数产品,InvivoChem推荐用DMSO配置母液 (比如:5、10、20mM或者10、20、50 mg/mL浓度),个别水溶性高的产品可直接溶于水。产品在DMSO 、水或其他溶剂中的具体溶解度详见上”溶解度 (体外)”部分;
2、如果您找不到您想要的溶解度信息,或者很难将产品溶解在溶液中,请联系我们;
3、建议使用下列计算器进行相关计算(摩尔浓度计算器、稀释计算器、分子量计算器、重组计算器等);
4、母液配好之后,将其分装到常规用量,并储存在-20°C或-80°C,尽量减少反复冻融循环。
计算结果:
工作液浓度: mg/mL;
DMSO母液配制方法: mg 药物溶于 μL DMSO溶液(母液浓度 mg/mL)。如该浓度超过该批次药物DMSO溶解度,请首先与我们联系。
体内配方配制方法:取 μL DMSO母液,加入 μL PEG300,混匀澄清后加入μL Tween 80,混匀澄清后加入 μL ddH2O,混匀澄清。
(1) 请确保溶液澄清之后,再加入下一种溶剂 (助溶剂) 。可利用涡旋、超声或水浴加热等方法助溶;
(2) 一定要按顺序加入溶剂 (助溶剂) 。
 Degarelix acetate hydrate
Degarelix acetate hydrate
 DDO-2728
DDO-2728
 Vatalanib hydrochloride (Vatalanib hydrochloride; PTK787 hydrochloride; ZK-222584 hydrochloride; CGP-797870 hydrochloride)
Vatalanib hydrochloride (Vatalanib hydrochloride; PTK787 hydrochloride; ZK-222584 hydrochloride; CGP-797870 hydrochloride)
 Tuspetinib hydrate (HM43239 hydrate)
Tuspetinib hydrate (HM43239 hydrate)
InvivoChem的所有产品仅用于作科学研究,不面向患者销售
Copyright 2020 InvivoChem LLC | All Rights Reserved 粤ICP备20063088号-1





























